Acute renal failure (ARF) in the ICU is a common problem. In fact, it is estimated that up to 25% of patients admitted to the ICU will develop ARF which carries a mortality rate estimated to be 40-50%. Initiation of acute hemodialysis (HD) or continuous renal replacement therapy (CRRT) requires prompt placement of temporary vascular access.
Prior to sticking your patient, here are a few important considerations.
Catheter Choice
- Material
- Polyurethane Catheter: Semi-rigid, most commonly inserted at the bedside.
- Somewhat thermoplastic, but once these catheters bend, they will likely remain bent – limiting flow.
- Remember – HD catheters are semi-rigid, so their tip should rest in their SVC (advancing too far could perforate right atrium or ventricle)
- Silicone: Very flexible, used more for tunneled catheters (usually by interventional radiology)
- Polyurethane Catheter: Semi-rigid, most commonly inserted at the bedside.
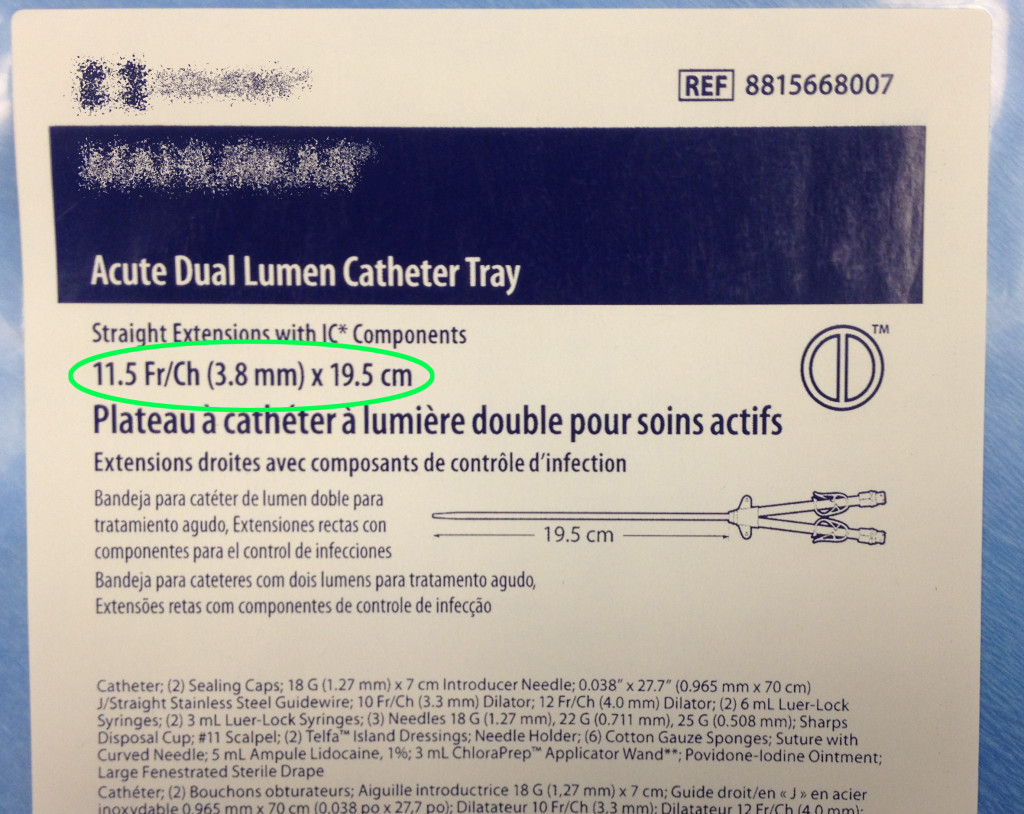
- Size
- Outer diameter varies between 11-14 French
- Larger diameter preferred
- However, larger diameter may increase risk of stenosis
- Length varies between 15 – 24 cm
- Right Internal Jugular: 12-15 cm
- Left Internal Jugular: 15-20 cm
- Femoral Vein: 19-24 cm
- Outer diameter varies between 11-14 French

Location
- Consider coagulopathy, morbid obesity, previous surgeries, altered anatomy, ability to tolerate lying flat, etc.
- Right IJ > Left IJ > Femoral > Subclavian
- Right Internal Jugular Vein: Preferred site
- More direct line to the caval-atrial junction = higher blood flow
- Less associated complications (kinking, obstruction, vein stenosis, etc.)
- Generally will use a 13.5 Fr, 15 cm catheter
- Left Internal Jugular Vein (2nd choice)
- Tortuosity can reduce flows
- Make sure to use a longer catheter (19.5 cm Quinton)
- Femoral Vein (3rd choice)
- Faster
- Reduce patient mobility
- Higher recirculation rates
- If using, make sure to use the longest possible catheter (24 cm Quinton) to make sure the tip reaches the distal IVC
- Pearl: If you find that your RRT Circuit is constantly shutting down, or having really low flows, check the HD catheter length. If the catheter tip is not long enough to reach the distal IVC, the RRT pump will often shut down secondary to inadequate flows.
- Just like with femoral CVC’s, femoral HD catheters do have a higher risk of infection and should only be used for a short period of time before being changed.
- *** Clarification (see comments from Dr. Weingart below): Important to note, in the short term (< 7 days) the risk of infection between different sites is probably no different.
- Note: In critically ill patients, usually we’d place a subclavian CVC because it has the lowest risk of infection. However, for temporary HD access, the SC vein should be avoided. Use of the subclavian for temporary HD catheters is associated with higher rates of central vein stenosis, which would affectively prevent the use of the ipsilateral arm as a site for long-term HD access (AV graft, fistula).
Duration
- Upper lines (IJ or subclavian): 3 weeks
- Femoral HD Catheters: 5 days
Catheter Insertion
- Stop doing them blind – Ultrasound guided insertion is the way to go (increases success rate, reduces hemo-/pneumothorax rates, etc.)
- Maximal sterile barrier precautions should be used
- Cover the site as you would a central line.
Complications
- Myth: Temporary, non-tunneled HD Catheters are less likely to get infected than CVC’s
- In fact, the use of noncuffed HD catheters is associated with substantial risk of infection (Maki, 2006)
- Non-cuffed HD Catheter Infection Rate: 4.8 BSIs per 1000 catheter-days
- Tunneled, cuffed HD line: 1.6 per 1000 catheter-days
- Compare with average CVC Infection rate: 2.7 per 1000 catheter days
- In fact, the use of noncuffed HD catheters is associated with substantial risk of infection (Maki, 2006)
- Malfunction
- Caused by thrombosis, kinking, malpositioning
- To prevent intraluminal thrombosis, catheter should be filled with an anticoagulant during interdialytic period
- Catheter tip positioning is KEY
- For upper, non-silicone lines the catheter tip should be at the junction of the SVC and the atrium.
- For femoral lines, the catheter tip should be resting in the distal IVC
References
- Schetz M. Vascular access for HD and CRRT. Contrib Nephrol. 2007;156:275-86.
- O’Grady N, Alexander M, Dellinger P, Gerberding JL, Heard SO, Maki DG, Masur H, McCormick RD, Mermel LA, Pearson ML, Raad II, Randolph A, Weinstein RA; the Healthcare Infection Control Practices Advisory Committee: Guidelines for the prevention of intravascular catheter-related infections. Infect Control Hosp Epidemiol 2002;23:759–769.
- Klouche K, Amigues L, Deleuze S, Beraud JJ, Canaud B: Complications, effects on dialysis dose, and survival of tunneled femoral dialysis catheters in acute renal failure. Am J Kidney Dis 2007;49: 99–108.
- Agarwal AK, Patel BM, Haddad NJ. Central vein stenosis: a nephrologist’s perspective. Semin Dial. 2007;20(1):53-62.
- Maki DG, Kluger DM, Crnich CJ. The risk of bloodstream infection in adults with different intravascular devices: a systematic review of 200 published prospective studies. Mayo Clin Proc. 2006;81(9):1159-71.
[author title=”About the Author”]