Today we are honored to have Dr. Wan-Tsu (Wendy) Chang, member of both the Neurocritical Care Department and the Emergency Department here at the University of Maryland. Dr. Chang has spent the last several years studying the best way to treat patients suffering from intractible status epilepticus. She has taken time from her busy schedule to share the many tips and tricks she has gained along the way. No matter what ICU you find yourself in, this lecture is a MUST LISTEN as often the most dangerous seizing patient is sitting right in front of you!
Overview of Status Epilepticus (SE):
- Three points to know:
- ↑ Morbidity and Mortality in the ICU population
- Goal is seizure cessation within 30 mins of onset
- WATCH for Non-Convulsive Status Epilepticus (NCSE) in the comatose, delirious, or recovering SE pts
- Worrisome facts:
- 1/2 of pts with SE have NO history of a seizure disorder
- TBI and Anoxia (#1 cause of mortality in SE) are very common presenting signs
- 30 day mortality- 19-27%
- Even if the pt survives- ↑ Epilepsy, Encephalopathy, Focal Neuro Deficits
- 50% of pts who present with SE will eventually develop NCSE
- >50% of NCSE are missed on a spot EEG
- >20% of NCSE are missed on 24 hour continuous EEG
- Time is brain!! – The longer the pt is in SE
- GABA receptors are down regulated (meaning benzos are less efficient)
- Neuronal transport proteins are upregulated (pumping Phenytoin out of the cells)
- NMDA receptors are upregulated (making Ketamine a viable treatment option)
- Definitions you MUST know:
- Status Epilepticus: convulsions > 5 mins in duration OR 2 or more sz episodes without a return to baseline
- Non-Convulsive Status Epilepticus: Sz w/o convulsions > 30 mins w/ EEG disturbance
- Refractory Status Epilepticus: SZ> 60 mins OR Sz despite therapeutic levels of 2 anti-epileptic drugs
- Super Refractory Status Epilepticus: Cont sz x 24 hrs following anesthetic measures
Treatment of Status Epilepticus (SE):
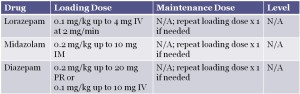
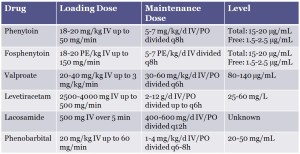
- First line
- Benzos, Benzos, BENZOS!
- #1 choice: Lorazepam – 4 mg IV to start with another 4 mg IV when needed
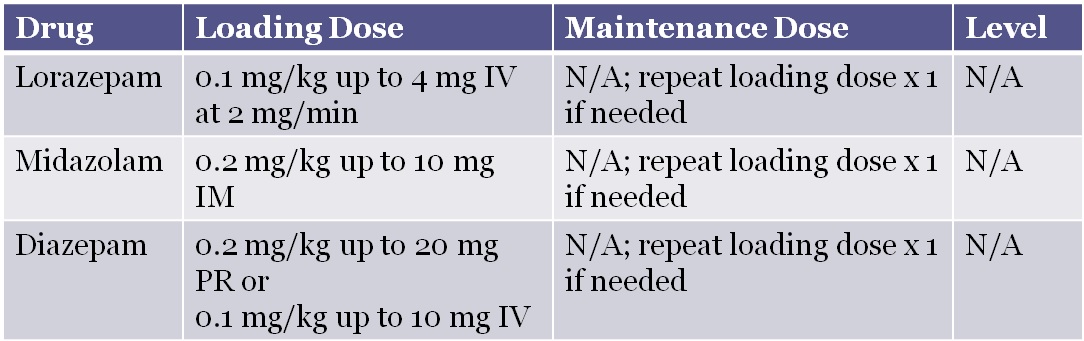
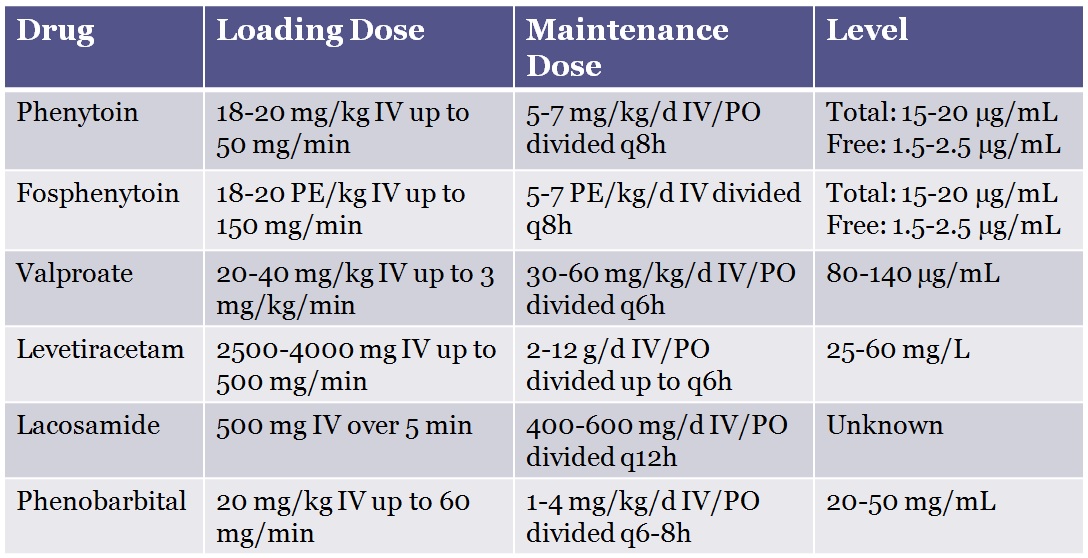
- Second Line
- Unknown, but a recent meta-analysis by Yasiry and Shorvon showed that Valproic Acid is slightly more effective then Phenytoin
- Regardless of what is used, watch for SEs: Hypotension for Pentobarb, Refractory/Withdrawal sz with Benzo drips
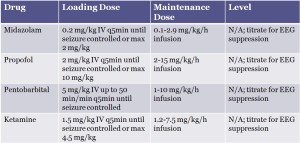
- Third Line
- Therapeutic induced coma for refractory or super refractory seizures
- End point of therapeutic coma: EEG sz control x 24-48 hours AND therapeutic levels of 2 anti-epileptic drugs

- Other treatments to try:
- Hypothermia
- Immunomodulation
- Surgical resection of seizure foci
- Inhaled anesthetics
- Ketogenic diet (difficult as most drips are in a glucose formula)
- Electric/Magnetic stimulation implants
Remember:
- Always suspect NCSE in the differential of AMS
- Always escalate from benzos when clinically needed!
Suggested Readings
- A. Fernandez, H. Lantigua, C. Lesch, B. Shao, B. Foreman, et al. High-dose midazolam infusion for refractory status epilepticus
Neurology, 82 (2014), p. 359 [Free Full Text] - Hocker S, Tatum WO, LaRoche S, Freeman WD. Refractory and super-refractory status epilepticus–an update.Curr Neurol Neurosci Rep. 2014 Jun;14(6):452. [PubMed]
- Yasiry Z, Shorvon SD. The relative effectiveness of five antiepileptic drugs in treatment of benzodiazepine-resistant convulsive status epilepticus: a meta-analysis of published studies. Seizure. 2014;23:167–74. [Free Full Text]
