Dr. Sam Galvagno is a Lieutenant Colonel in the US Air Force who is an expert in anesthesia critical care, airway management, critical care education, published in JAMA, and a black belt in Tae Kwon Do to boot. Did I mention he earned a PhD in Clinical Investigation? This short talk is JAM PACKED with clinical pearls. Needless to say, Dr. Galvagno owns the resuscitation room in more ways than one and we were lucky enough to have him come and give us his opinions on induction agents for the critically-ill.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS
Key points
- “Earning the anesthetic,” applies to the concept that a patient’s physiology must be able to handle the prescribed dose of induction agent. Shocked patients usually require a significantly reduced dose of anesthetic to avoid adverse effects of hypotension and cardiac depression.
- Critical for anyone involved in airway management to do at least 3 things
- BEFORE you begin your RSI, commit to a definitive airway
- Gather extra hands and delegate tasks. Focus on doing one thing and one thing only.
- Your equipment should be prepared and proximal
If it isn’t within 3 feet of you, it might as well be on MARS
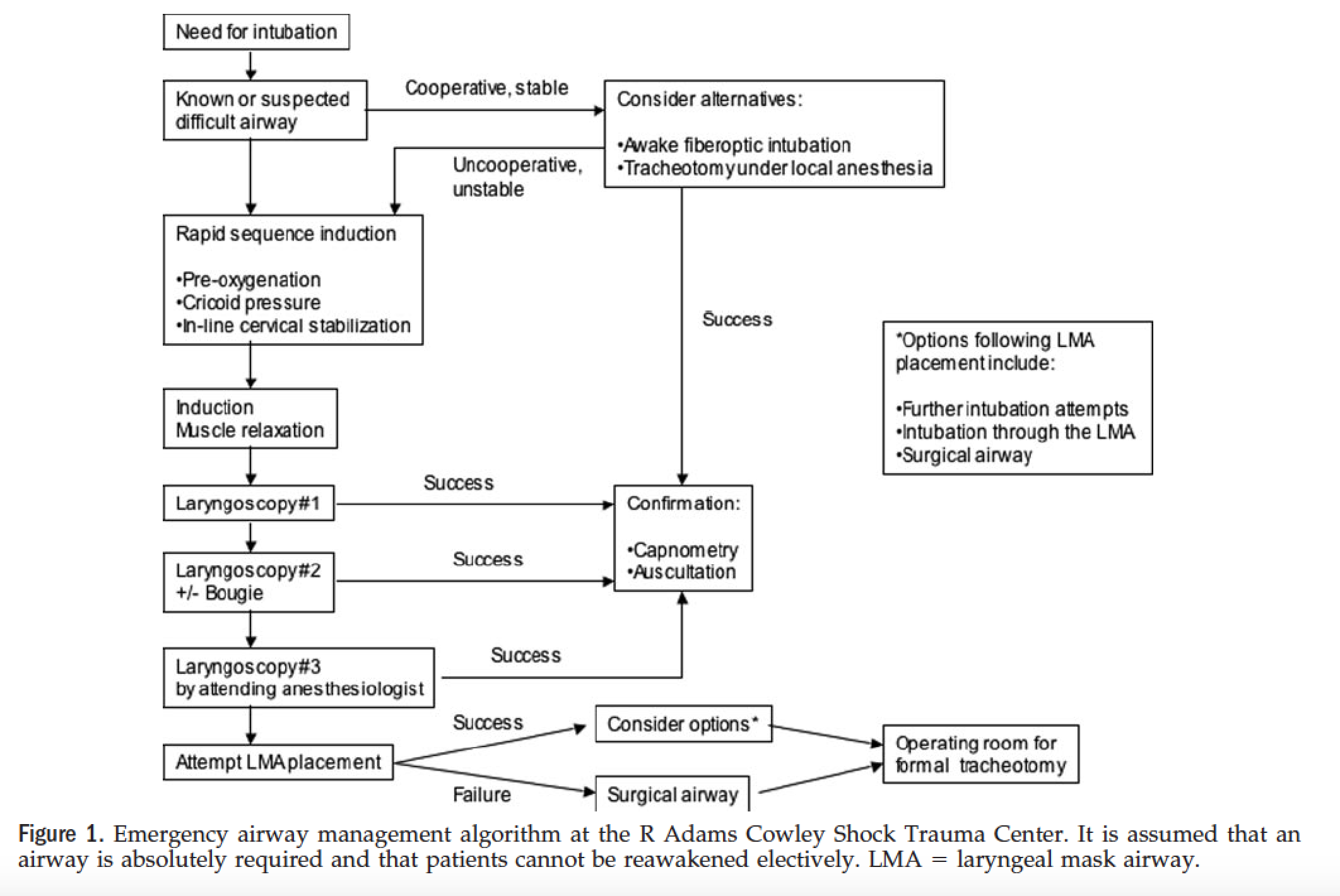
STC Airway Algorithm
Paralytics
- The Roc vs. Sux debate goes on…
- Personal preference for Rocuronium, but you still need to know how to effectively use Sux (and even Vecuronium!) as a back up plan (drug shortages)
- Sux vs. Roc Cochrane Review – Rocuronium was underdosed in a majority of these studies, which is why sux may have looked better.
Induction Agents
Etomidate
- Dose: 0.2 – 0.3 mg/kg Ideal Body Weight
- Adverse reactions: Emetic, really not as hemodynamically neutral as we think.
- Adrenal insufficiency?
- May be a signal, but unsure if there is clinical significance. Studies indicating AI reasonably criticized.
- Wagner, 2014 – Probably one of the most well done studies showing no AI.
Propofol
- Dose: 0.5 mg/kg or LOWER
- Dose highly dependent on hemodynamic status.
- Known to highly reduce SVR, BP, ICP, and is a cardiac depressant.
- Probably should administer in 10 mg boluses if giving to a critically ill patient
- Bottom line: Probably shouldn’t be using in the acutely-ill patient due to known side effects.
Ketamine
- Dose: 0.5 – 2 mg/kg IV, standard dose of 1 mg/kg usually adequate
- Prepare those around you for the patient to dissociate, not fall asleep.
- Benefits: Patient continues spontaneous breathing
- Pitfalls
- Ketamine is a direct myocardial depressant, so be cautious when inducing with ketamine in the patient with a low EF. Effects are usually balanced by increased catecholamine release.
- Beware the patient with prolonged shock or who is catecholamine deplete – you won’t see that BP bump you’re used to.
- Primary drug of choice for a majority of emergency airways today
Suggested Readings
- El-orbany M, Connolly LA. Rapid sequence induction and intubation: current controversy. Anesth Analg. 2010;110(5):1318-25.
- Stollings JL, Diedrich DA, Oyen LJ, Brown DR. Rapid-sequence intubation: a review of the process and considerations when choosing medications. Ann Pharmacother. 2014;48(1):62-76.
- Sikorski RA, Koerner AK, Fouche-Weber, LY, Galvagno SM. Choice of General Anesthetics for Trauma Patients. Curr Anesthesiol Rep (2014) 4:225–232. [Download pdf]
- Weingart S. Podcast 104 – Laryngoscope as a Murder Weapon (LAMW) Series – Hemodynamic Kills. http://emcrit.org/podcasts/intubation-patient-shock/