Managing complex patients with ARDS can be challenging. Many believe the Berlin criteria we use to identify ARDS are largely confounded and often identify the disease too late. Additionally, how do you manage the patient who’s intravascularly depleted but is drowning from pulmonary edema? (Classic – they are wet and dry!!) What if there was a way to identify the patient developing ARDS before a blood gas or chest x-ray? Or even better, objectively treat their excessive extravascular lung water? We were fortunate enough to have Dr. Nielsen return to speak on this interesting topic. Dr. Nielsen is an intensivist who has a great deal of experience PiCCO and using extravascular lung water estimates to guide complex therapies in patients with ARDS.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS
Extravascular Lung Water (EVLW) & Transpulmonary Thermodilution (TPTD)
Written summary by Dr. Nikki Naderi
Definition and Measurement
- EVLW: all the fluid in the lungs that is not intravascular or intrapleural i.e. surfactant, edema
- Consists of 20-25% of the total fluid in the lungs
- Normal: < 7 ml/kg
- Measured by:
- Gravimetry- gold standard for measurement, however can be only done ex-vivo, the lung is weighed both wet and dry, the difference in the weight is EVLW
- TPTD: both double indicator (thermo-dye) and single indicator (thermos) methods correlate closely with gravimetry and can by down in-vivo
- In a single indicator thermodilution, cold water is injected through an internal jugular or subclavian veins. An intrarterial thermister placed in the femoral artery measures the change in blood temperature and plots it against time.
- From these measurements EVLW can be calculated
PiCCO Parameters
- Cardiac output (CO) & index (CI)
- Volumetric Preload (GEDV) & Index (GEDI)
- Lung water (EVLW)
- Afterload (SVRI)
- Contractility (CFI)
- Volume responsiveness (SVV/PPV)
Clinical Applications
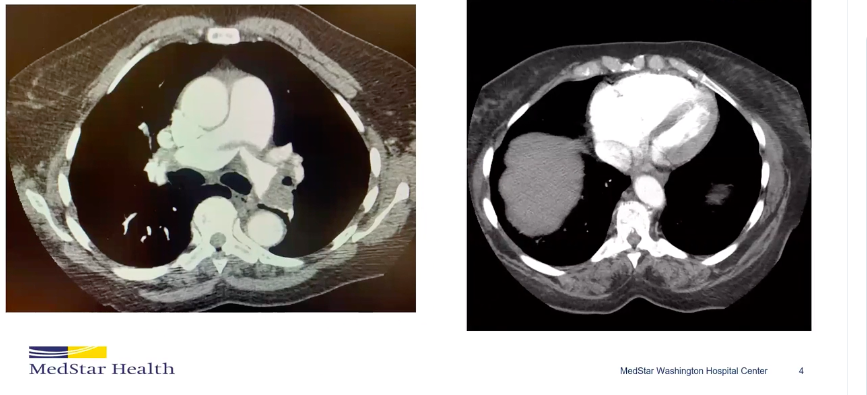
- Diagnosis, prognosis and treatment guidance in ARDS
- In multiple studies EVLW has been found to have a linear correlation with lung weight
- An EVLW of about 15 mL/kg was 99% specific for diffuse alveolar damage
- Predicts onset of acute lung injury (ALI) before traditional parameters to diagnose ALI/ARDS such as hypoxia and CXR findings
- EVLW when indexed to pulmonary blood volume can discriminate hydrostatic edema (due to cardiac causes) from ARDS
Prognosis
- For every increase of 1 mL/kg of EVLW, there is a 7% increase risk of death and an EVLW of greater than 21 mL/kg has a mortality of >70%
Treatment
- EVLW has been shown to be a better surrogate for degree of pulmonary edema in ARDS than wedge pressure, thereby a more accurate guide in treatment and diuresis of patients with ARDS

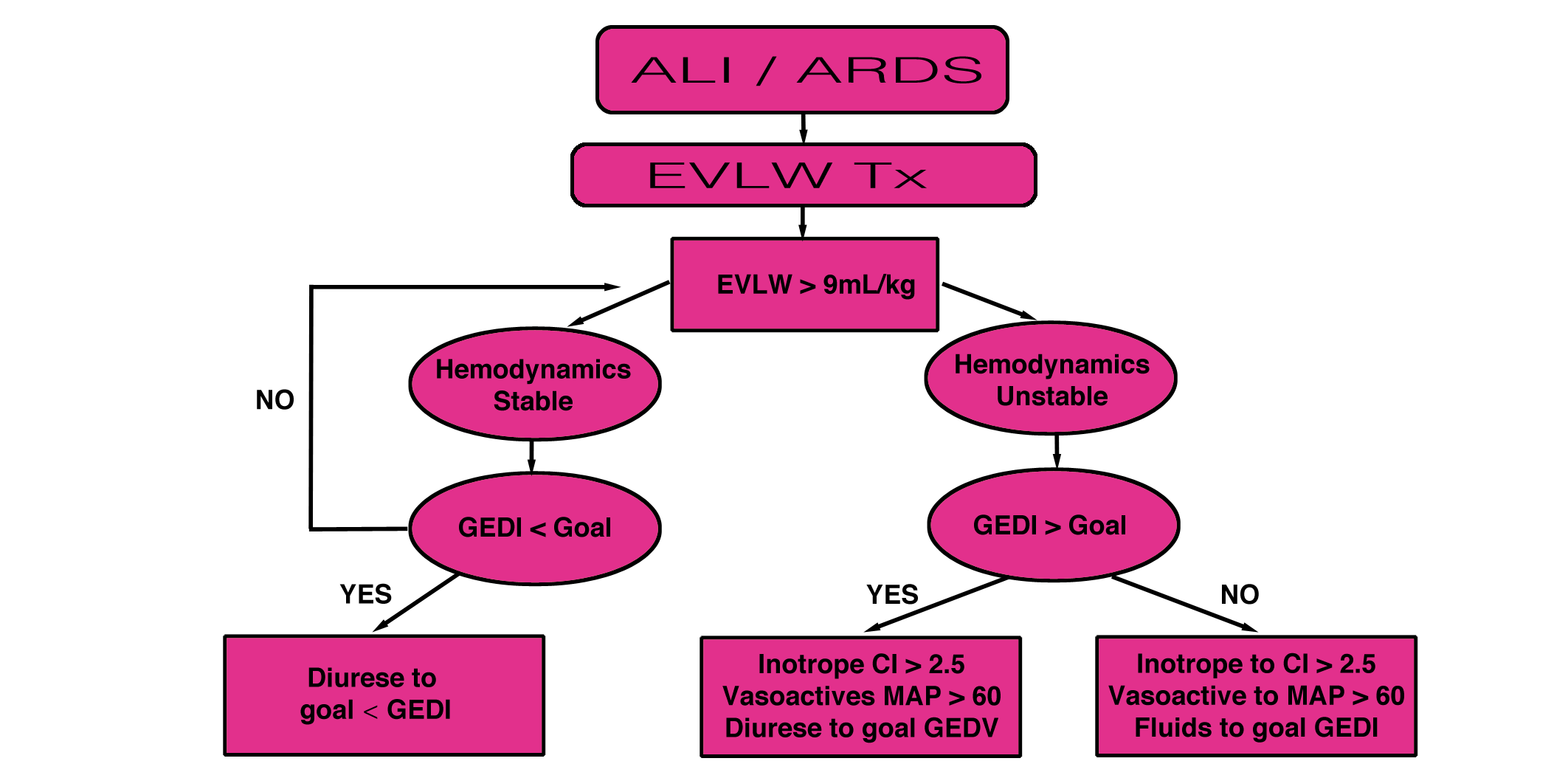
Potential Goal Directed Management Algorithm
Limitations
- The measurement of EVLW can be underestimated in patients with underlying lung disease, focal lung disease, shunt, high PEEP on the ventilator, pulmonary vascular obstruction and a cardiac index of less than 1.5
- Hemodynamic monitoring unreliable in patients with arrhythmias, right heart failure, and require controlled ventilation
Additional Reading
- Tagami T, Sawabe M, Kushimoto S, et al. Quantitative diagnosis of diffuse alveolar damage using extravascular lung water. Crit Care Med. 2013;41(9):2144-50. [PubMed Link]
- Jozwiak M, Silva S, Persichini R, et al. Extravascular lung water is an independent prognostic factor in patients with acute respiratory distress syndrome. Crit Care Med. 2013;41(2):472-80. [Open Access Link]
- Sánchez M, García-de-lorenzo A, Herrero E, et al. A protocol for resuscitation of severe burn patients guided by transpulmonary thermodilution and lactate levels: a 3-year prospective cohort study. Crit Care. 2013;17(4):R176. [Open Access Link]