[x_text]Today we are fortunate to have Dr. Joseph R. Shiber, an Associate Professor in the Departments of Emergency Medicine and Surgical Critical Care at the University of Florida College of Medicine. Dr. Shiber also acts as the Co-Director of the Neuroscience ICU and attends in the SICU/TICU. And if that wasn’t enough, he has also has the distinct pleasure of the being in the FIRST graduating class of the EM/IM/CCM program at the University of Maryland! This is a talk that you CANNOT miss if you ever plan to encounter COPD or CHF in your patient population. [/x_text]
[x_text][/x_text][x_text]
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS
[/x_text][x_text class=”left-text “]
Lecture Summary
- (Pearls provided by Dr. Faith Armstrong: 1st year CCM Fellow at the UMMC)
Goals of Mechanical Ventilation:
- Improve gas exchange
- Assist work of breathing
- Tx neuromuscular weakness (must determine reversible vs non-reversible!)
- Prevent/improve atelectasis
- For decreased ventilator drive
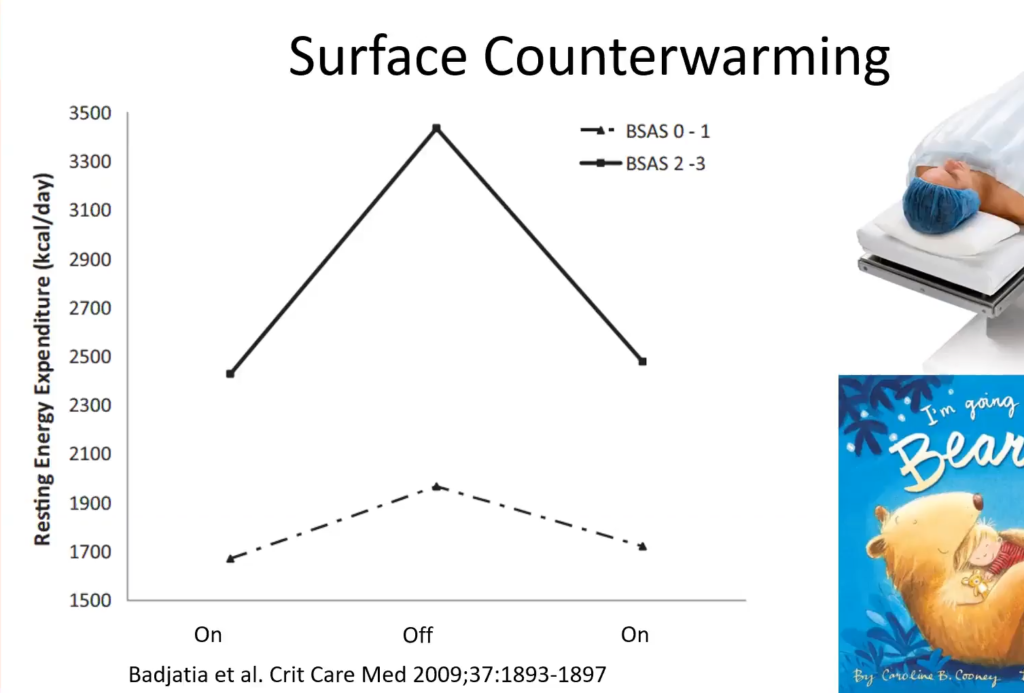
- Decrease O2 consumption
- Airway protection (cannot do on NIPPV)
- To permit sedation/paralysis (cannot do on NIPPV)
Respiratory Failure Candidates:
- Hypoxemia: pO2<50-60
- Hypercarbia: pCO2>50 AND pH<7.32
- Mixed: BOTH (post-op, often due to atelectasis)
- Origin of symptoms: Circulatory shock
Pressure-Volume Relationship (figure from Papadakos and Lachmann, Crit Care Clin 2007)

- Patients we help with NIPPV are at both ends of the curve
- Those on the left/lower end are helped by re-inflating collapsed lung with PPV
- Those on the right/upper portion of the curve are helped by improving expiratory flow, as in COPD/Asthma (overinflated states)
Pulmonary Effects
- Alveolar recruitment
- Improved V/Q mismatch (but beware of increasing dead space with hyperinflation as perfusion can be compromised!)
- ↓ auto-PEEP
- ↑ airflow
- ↓ workload
- DRAWBACK: Worsen secretion clearance
Hemodynamic Effects

- ↓ preload*
- ↓ LV afterload*
- ↑ contractility*
- “LVAD” effect: by assisting all three CO will increased; however in cases of hypovolemia, NIPPV can DECREASE CO because of its deleterious effect on preload, and thus decrease O2 delivery to tissue
- ↑ RV afterload with R>L septum shift
- DOWNSIDE: Increased dead space (hyperinflated alveoli can compress vasculature)
Overall Benefits
- Improved subjective symptoms
- ↓ rate of intubation
- ↓ mortality
- ↓ morbidity (sedation, VAP, RSI)
- ↓ ICU LOS and costs
- ** Limited window to use (better success early!) **
Indications
- CHF/acute cardiogenic pulmonary edema
- Prevent intubation; better outcomes; improvement in SaO2, RR, SOB; no incr risk of MI
- COPD/Asthma
- Prevent intubation; better outcomes; improvement in PacO2
- CAP in the immunocompromised (↓ VAPs)
- REVERSIBLE Neuromuscular disease (myasthenia gravis, GB…use in ALS is controversial because it is not reversible)
- DNR patients (for relief of dyspnea)
- OSA/Pickwickian
- Delayed sequence intubation (optimize your patient prior to intubation)
- Post-extubation airway edema (essentially stenting the airway open)
- Planned step of MV weaning (“extubate to NIPPV”)
Contraindications
- Respiratory arrest
- Hemodynamically unstable
- Uncooperative/agitated (usually signals severe hypoxemia)
- Aspiration risk
- Unable to fit mask properly (trauma, burns)
- High-grade upper airway obstruction
Poor Candidates for NIPPV
- ARDS (except in delayed sequence intubation) – 80% failure rate!
- Spinal Cord Injury (not a reversible NM disorder)
- UGIB (airway not protected)
- Shock w/ MOF (NIPPV does not fully replace work of breathing)
- Vomiting patients, especially if restrained
Complications
- Facial pressure injury (avoid with scheduled breaks off mask)
- Gastric distention when PIP >25
- Secretion retention/plugging
- Aspiration (usually due to MS decline and/or restraints)
- Delay in intubation as the primary process worsens
Tips/Tricks
- Best candidates: alert/cooperative, w/ strong cough, good nutritional status , and with low APACHE II scores
- NIPPV s best when applied EARLY; most of the patients who fail NIPPV failed because WE waited too long to apply it
- Ketamine and Dexmedetomidine are best for sedation (no resp inhibition)
- Must reassess s/p 30-60 minutes for improvement
- Don’t delay intubation if it’s needed, especially with ARDS patients. Act before they decompensate!
- NGT are not necessary as gastric distention isn’t an issue until PIP is >25
- Placement can actually worsen the picture since the LES is opened once NGT is placed!
- Don’t forget about HFNC (vapotherm)! Gives CPAP ~5cmH2O
[/x_text]
[x_text]Suggested Reading
- AlYami MA, AlAhmari MD, Alotaibi H, AlRabeeah S, AlBalawi I, Mubasher M. Evaluation of efficacy of non-invasive ventilation in Non-COPD and non-trauma patients with acute hypoxemic respiratory failure: A systematic review and meta-analysis. Ann Thorac Med. 2015 Jan-Mar;10(1):16-24. [Pubmed Link]
- Stefan MS, Nathanson BH, Higgins TL, Steingrub JS, Lagu T, Rothberg MB, Lindenauer PK. Comparative Effectiveness of Noninvasive and Invasive Ventilation in Critically Ill Patients With Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Crit Care Med. 2015 Jul;43(7):1386-94 [PubMed Link]
- Gray A, Goodacre S, Newby D, Masson M, SampsonF, Nicholl J, for the 3CPO Trialists. Noninvasive Ventilation in Acute Cardiogenic Pulmonary Edema. N Engl J Med 2008; 359:142-15. [NEJM Link]
[/x_text]