Today we are fortunate that Dr. Daniel Herr, Chief of Surgical Critical Care services and Director of the Cardiac Surgery/Heart-Lung Transplant ICU here at the University of Maryland and overall critical care genius. Today Dr. Herr tackles a topic that often stares us right in the face, offering us all the knowledge we could ever need to treat patients, and yet we ignore it: End Tidal CO2!! This is a talk that you NEVER knew you needed until you hear it. Trust me, this is 45 minutes your patients cannot live without!
Clinical Pearls (assisted by Dr. Lino Rafael O. Trinidad)
#1 concept: Will be the first warning of trouble in a struggling patient!
Capnography → LEAVE IT ON!! If esophageal, will go BACK to purple
- Is the immediate picture of ventilation (SpO2 delayed)
- Hypoventilation occurs 1-2 minutes before hypoxemia
- Ways of Measuring (Is the LAW for conscious sedation)
- POC addition to ETT (standard intubation equipment)
- Sidestream- can add dead space; can underestimate CO2
- Mainstream- T-piece adaptor at the airway opening; does not add dead space
- Mass Spectrometry- CO2 eliminated / O2 consumed
CO2 Waveform
- Evaluate for:
- Height
- Frequency
- Rhythm
- Baseline
- Shape
- Systematic Approach
- Is CO2 present (waveform)
- Is the baseline zero
- Evaluate the:
- Expiratory upstroke: steep, sloping, prolonged
- Expiratory (alveolar) plateau: flat prolonged, notched, or sloping
- Inspiratory downstroke: steep sloping or prolonged
- Just read the number
- Check ABG (Try to match the PaCO2, if its not within 5 a problem)

- Alpha angle: amount of V/Q mismatch
- Beta angle: if >90 degrees → rebreathing occurring
Evaluation of waveform abnormalities:
- Waveform regular shape
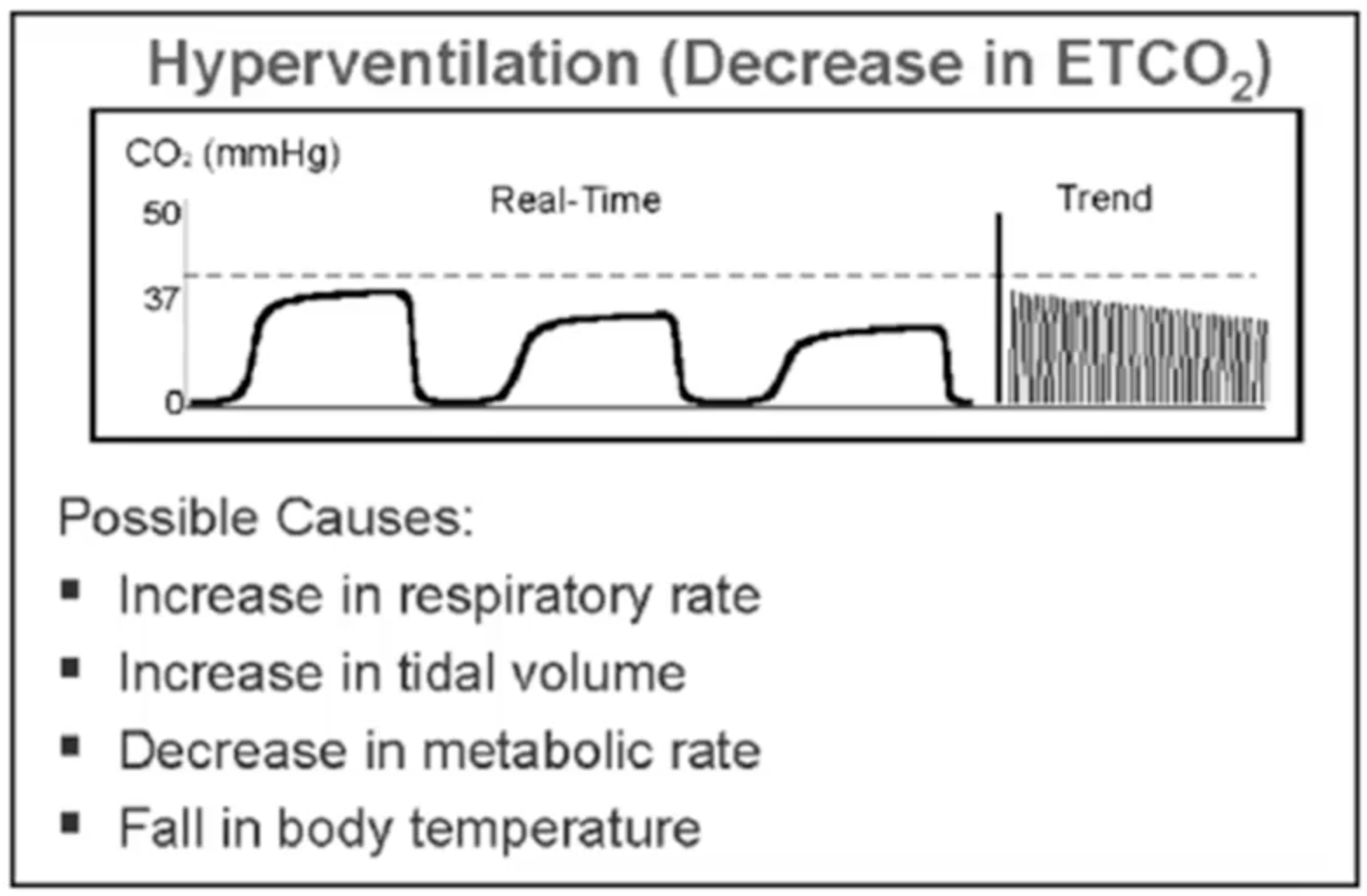
- Plateau below normal = CO2 deficiency
- Hyperventilation
- Decreased pulm perfusion
- Hypothermia
- Decreased metabolism
- Plateau above normal = CO2 excess
- Hypoventiltion
- Absorption of CO2 during laparoscopy
- Fever
- Dietary excess
- Sudden increases: sodium bicarb use, release of tourniquet
- Watch for Trends:
- Plateau below normal = CO2 deficiency
Special uses:
- Assessing Intubation and Ventilation
- 100% specific
- Facemask can force some pharyngeal air into stomach
- Esophageal intubation may be positive for CO2 (usually less than 10, decreases over breaths)
- Watch out for plug, kink, apnea, severe bronchospasm
- 100% specific
- ETCO2 and CO
- CO largely affect ETCO2 in dynamic situations, not when stable
- ETCO2 < 10 after 20 mins of CPR associated with a very high mortality
- Must make sure adequate compressions before judging ETCO2
- Dead Space i.e. Altered CO2 clearance
- Hypercapnea with adequate ventilation implies dead space
- Bohr-Enghoff Equation; Dead space = (PaCO2 – PECO2) / PaCO2
- Normal dead space is 2ml/kg
- Can be also calculated via Volume Capnogram
- Ventilator Adjustment
- Increase PEEP if gradient too high
- Useful for weaning vent once gradient is established
- Measure ETCO2 every time you get ABG
- Increase PEEP if gradient too high
- ARDS (?Dead Space Disease)
- TV distributed to poorly or non-perfused parts:
- Microemboli
- Endothelial damage
- Non-survivors have higher dead space, can be prognostic
- Serial measurement of deadspace for progression
- TV distributed to poorly or non-perfused parts:
- PE
- Hypoxia, clinical scenario
- 13-20% drop in dead space = CTA immediately
- Good NPV (100%); PPV (66%)
- Ventilator Weaning
- Obtain a gradient every AM (Volumetric would be more helpful)
- ETCO2 + RSBI is indicative of the proper score for extubation
- VA ECMO Weaning
- ↓ECMO flow by 40% → ETCO2
- ETCO2 will changed steeply with a flexion point (good symbol of coming off VA ECMO)
- ↓ECMO flow by 40% → ETCO2
Suggested Reading
- Checketts MR, Alladi R, Ferguson K, Gemmell L, Handy JM, Klein AA, Love NJ, Misra U, Morris C, Nathanson MH, Rodney GE, Verma R, Pandit JJ; Association of Anaesthetists of Great Britain and Ireland. Recommendations for standards of monitoring during anaesthesia and recovery 2015: Association of Anaesthetists of Great Britain and Ireland. Anaesthesia. 2016 Jan;71(1):85-93.[PubMed link]
- Thomas AN, Harvey DJR, Hurst. Standards for Capnography in Critical Care – The Intensive Care Society Guidelines 2014. [ICS Link]
- Nassar BS, Schmidt GA. Capnography During Critical Illness. Chest. 2016 Feb;149(2):576-85.[Pubmed Link]
- Monnet X, Bataille A, Magalhaes E, Barrois J, Le Corre M, Gosset C, Guerin L, Richard C, Teboul JL. End-tidal carbon dioxide is better than arterial pressure for predicting volume responsiveness by the passive leg raising test. Intensive Care Med. 2013 Jan;39(1):93-100.[PubMed Link]