Rory Spiegel, MD, Critical Care Medicine Fellow, Division of Pulmonary & Critical Care Medicine and Clinical Instructor, Department of Emergency Medicine at the University of Maryland SOM, presents the weekly multi-departmental critical care fellows’ lecture on “Starling, Guyton, and Ultrasonographic Findings of Venous Excess.”
Lecture summary written by Robert Brown, MD
A growing body of evidence is calling for thoughtful use of IV fluids
- The FEAST trial from Andrews et al. Effect of an early resus protocol on in-hospital mortality among adult with sepsis and hypotension. JAMA. 2017;318(13):1233-1240
- The CLASSIC trial from Hjortrup et al. Restricting volumes of resus fluid in adults with septic shock after initial management. Intensive Care Med 2016 42:1695-1705
- Comparison of two fluid management strategies in acute lung injury by the national heart lung and blood institute acute respiratory distress syndrome clinical trials network N Engl J Med 2006;354:2564-75.
- ANDROMEDA trial from Hernandez et al. Effect of a resus strategy targeting peripheral perfusion status. JAMA. 2019;321(7):654-664
Moving from the concept of fluid responsiveness to the concept of fluid tolerance
- A healthy person is fluid responsive but driving fluid volume high enough to no longer be responsive is to overload them
- IVF do not stay intravascular for long. Only 15-30 minutes
- Giving fluid quickly corresponds to 3rd spacing even faster.
The physiologic basis for fluid tolerance
- Mean systemic pressure is 7mmHg on the venous side (that’s the pressure exerted by the walls of the veins pressing on the blood and it competes with the pressure in the right ventricle)
- Therefore, the right ventricle changes shape to accommodate volume without changing pressure
- In sepsis you lose venous tone, and thus pressors can help
- Most of the filling of the right atrium occurs during right ventricular systole but when you have venous excess, you end up with more backflow into the venous system instead of forward flow
Measuring with Ultrasound
- Hepatic vein – blood is flowing away from the probe and toward the
heart until the atrial kick briefly sends it retrograde
- The hepatic flow waveform looks just like the CVP tracing, you can see the atrial kick, filling during right ventricular systole, and then diastolic filling
- With venous congestion the systolic filling decreases and diastolic filling increases. When severe, the waves fuse and all forward flow is happening in right ventricular diastole
- Portal vein – thicker walls, also flows away from the probe,
toward the heart
- Flow is monophasic until you get venous excess – then you see pulsatility and when very severe there is backflow
- Portal pulsatility index = (peak – trough)/peak and there is a continuum, but 20% is a sign of pronounced pulsatility
- Renal vein
- Normal wave form shows increase in flow with systole and flow decreases in diastole but with greater congestion there is biphasic venous flow with systolic flow, then stop in flow, then diastolic flow and as congestion worsens, the systolic flow shrinks until all you have is diastolic flow
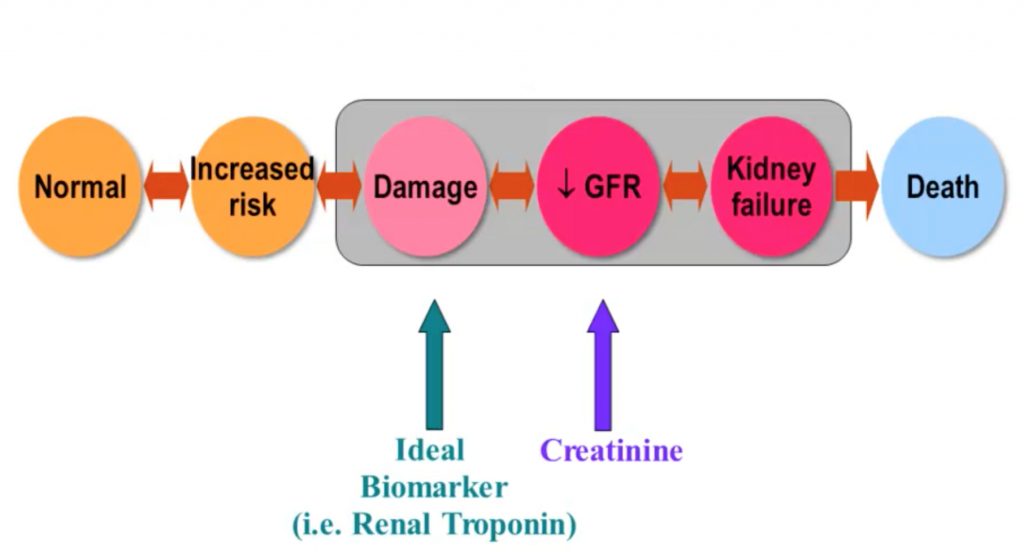
- Seeing biphasic flow predicts acute kidney injury (AKI)
- Beaubien-Souligny W, et al. The Association Between Pulsatile Portal Flow and Acute Kidney Injury after Cardiac Surgery: A Retrospective Cohort Study. J Cardiothorac Vasc Anesth. 2018;32(4):1780-1787
- Lida N, et al. Clinical Implications of Intrarenal Hemodynamic Evaluation by Doppler Ultrasonography in Heart Failure. JACC Heart Fail. 2016 Aug;4(8):674-82
Practical Points
- Once you complete the venous exam described above (the right-sided heart exam you could call it), look at the cardiac exam (the left sided heart exam, like the VTI),
- Septic patients – you can look at the venous side and determine when fluid will be harmful
- Neurosurgery and surgery patients in general will very likely need more fluid and their disease process is different – look at the arterial side
References
- Beaubien-Souligny, William, et al. “Extracardiac signs of fluid overload in the critically ill cardiac patient: a focused evaluation using bedside ultrasound.” Canadian Journal of Cardiology 33.1 (2017): 88-100. https://doi.org/10.1016/j.cjca.2016.08.012
- Iida, Noriko, et al. “Clinical implications of intrarenal hemodynamic evaluation by Doppler ultrasonography in heart failure.” JACC: Heart Failure 4.8 (2016): 674-682. https://doi-org.proxy-hs.researchport.umd.edu/10.1016/j.cjca.2016.08.012
- Tang, WH Wilson, and Takeshi Kitai. “Intrarenal venous flow: a window into the congestive kidney failure phenotype of heart failure?.” (2016): 683-686. https://doi-org.proxy-hs.researchport.umd.edu/10.1016/j.jchf.2016.05.009
- Funk, Duane J., Eric Jacobsohn, and Anand Kumar. “Role of the venous return in critical illness and shock: part II—shock and mechanical ventilation.” Critical care medicine 41.2 (2013): 573-579. https://doi-org.proxy-hs.researchport.umd.edu/10.1097/CCM.0b013e31827bfc25
- Beaubien-Souligny, William, et al. “The association between pulsatile portal flow and acute kidney injury after cardiac surgery: a retrospective cohort study.” Journal of cardiothoracic and vascular anesthesia 32.4 (2018): 1780-1787. https://doi-org.proxy-hs.researchport.umd.edu/10.1053/j.jvca.2017.11.030
- Funk, Duane J., Eric Jacobsohn, and Anand Kumar. “The role of venous return in critical illness and shock—part I: physiology.” Critical care medicine 41.1 (2013): 255-262. https://doi-org.proxy-hs.researchport.umd.edu/10.1097/CCM.0b013e3182772ab6
Uploaded by Sami Safadi, MD
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS