Samuel M. Galvagno Jr., DO, PhD, MS, FCCM, Associate Professor of Anesthesiology at the University of Maryland SOM & Associate Director, Maryland Critical Care Network at UMMC and Ross Carpenter, MD, Fellow in Cardiothoracic Anesthesia at the University of Maryland, present the weekly multi-departmental critical care fellows’ lecture on “Molecular Adsorbent Recirculating System: Life on MARS.”
Lecture Summary by Dr. Erik Manninen
Introduction
- Liver transplant is the second most common transplanted organ after kidney. <10% of global needs are met.
- Molecular adsorbent recirculating system (MARS) is an artificial liver support system that was developed in 1993 in Germany and became commercially available in 1999.
- It removes toxins that CRRT does not (although MARS is used in conjunction with CRRT).
- MARS is used as a bridge to transplant or a bridge to recovery. It is expensive and typically involves 3 sessions at a minimum, which costs about $45,000.
- Used successfully to bridge three patients to transplant that suffered heat stroke.
System Components
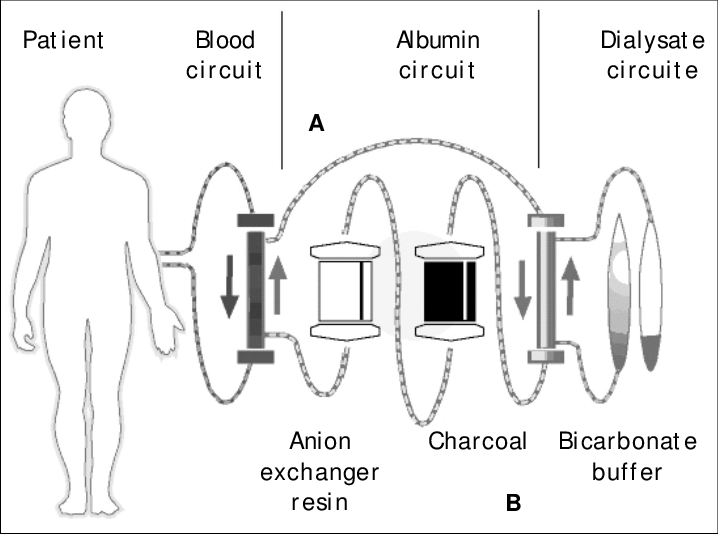
- The system uses three different circuits: blood, albumin and low-flux dialysis.
- First, blood is dialyzed against a human serum albumin dialysate solution
- Then, the albumin dialysate is regenerated in a close loop in the circuit by:
- passing through a low-flux dialysis filter against a standard dialysis fluid to clear water-soluble toxins
- passing through two different adsorption columns: activated charcoal to clear protein-bound substances and cholestyramine & an anion-exchange resin to clear anionic substances
- For one session 100g of 25% albumin is used.
Indications
- APAP overdose with one or more: INR>2.5, tbili>3, pH<7.3, and lactate >6mmol/L.
- Acute fulminant liver failure in a transplant candidate
- Acute on chronic liver failure in a listed transplant candidate
- Primary non-functioning post liver transplant and one or more of the following:
- listed for re-transplant,
- UNOS criteria for PNF
- hepatic artery thrombosis
- INR.2, lactate >6, and clinically deteriorating
- Patients with multiple organ failure on a case to case basis
Other Considerations
- N-acetylcysteine dosing should be doubled while on MARS. Other protein bound drugs also need to have dose adjustment and should be reviewed and your clinical pharmacist can be a big help with your patient while on MARS.
- Efficacy of MARS is judged on improving clinical parameters like decreasing dose of vasoactive medicines and improving mental status.
- There may be a role of using MARS to speed recovery of patients with acute liver failure as well, which allows earlier hospital discharge and doesn’t tie up a potential organ, which could be transplanted to a patient who truly needs it.
- While there are no precise recommendations on the effective timing of initiation of artificial liver support systems they can be helpful in select cases.
References
- Mitzner, Steffen R. “Extracorporeal liver support-albumin dialysis with the Molecular Adsorbent Recirculating System (MARS).” Annals of hepatology 10.S1 (2016): 21-28. https://www-ncbi-nlm-nih-gov.proxy-hs.researchport.umd.edu/pubmed/21566251
- Hanish, Steven I., et al. “Molecular adsorbent recirculating system effectively replaces hepatic function in severe acute liver failure.” Annals of surgery 266.4 (2017): 677-684. https://www.ncbi.nlm.nih.gov/pubmed/28692474
- He, Guo-Lin, et al. “Meta-analysis of survival with the molecular adsorbent recirculating system for liver failure.” International journal of clinical and experimental medicine 8.10 (2015): 17046. https://www.ncbi.nlm.nih.gov/pubmed/26770295
Uploaded by Sami Safadi, MD
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS