This week’s lecture was an introduction to the Left Ventricular Assist Device given by Dr. Gautam Ramani. In this talk Dr. Ramani discusses the fundamentals in deciding which patients should be considered for VAD placement, the different types of VADs, and finally spends the remainder of his time discussing the basics of VAD management. Do you have a differential for the patient who is alarming with an acute power reduction? What complications do you need to worry about? Lots of ground to cover here – this will be the first of a number of VAD posts we’ll have throughout the year – so sit back and relax for part 1.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS
Pearls
Risk Assessment for VADs
- Beware of the normotensive patient in acute heart failure – these patients have a high mortality and may need to be considered for a VAD.
- The ADHERE prediction model for in-patient mortality – watch the blood pressure and renal function
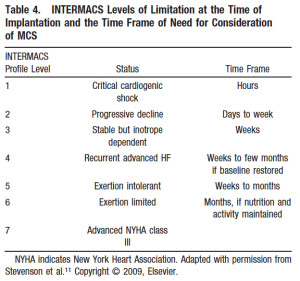
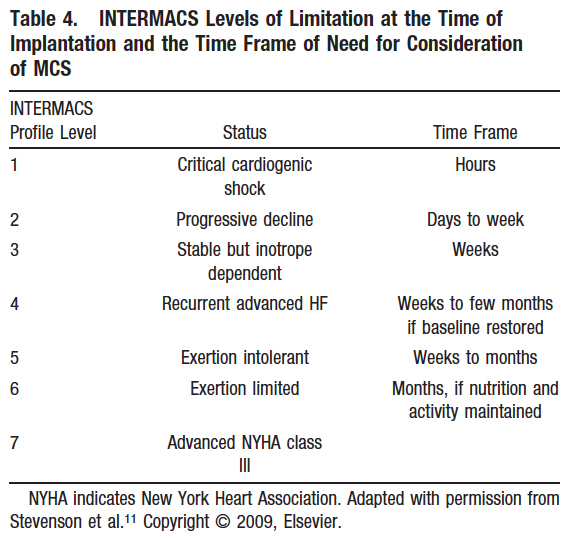
- Optimal timing of VAD placement
Tenets of Management
- All VADs are pre-load dependent – make sure the tank is full in the patient with a low MAP.
- VADs are ECG independent, unlike balloon pumps, ICDs, and other types of mechanical support.
- VADs are extremely afterload sensitive – large increases in BP will decrease pump flow/output.
- Rule of thumb – first assessment – listen for the hum of the VAD motor to ensure it is working
- VADs have 3 major variables:
- Speed
- Flow
- Power
- For any given speed, there should be an appropriate power output
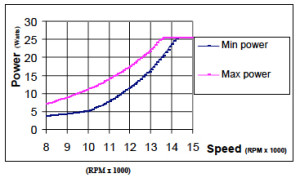
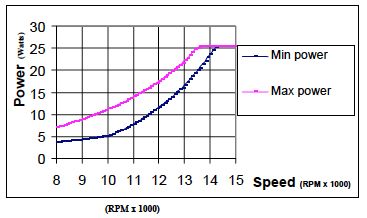
- Changes in POWER can indicate a number of things
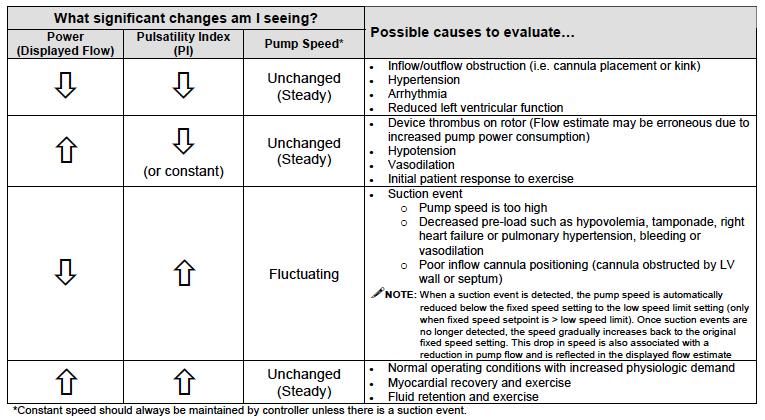
- Pulsatility index = ([Max Flow] – [Min flow]) / [Average Flow]
Stay tuned for more on the crashing VAD patient and what you need to look out for next.
References