Today we are fortunate that Dr. Daniel Herr, Chief of Surgical Critical Care services and Director of the Cardiac Surgery/Heart-Lung Transplant ICU here at the University of Maryland and overall critical care genius. Today Dr. Herr tackles a topic that often stares us right in the face, offering us all the knowledge we could ever need to treat patients, and yet we ignore it: End Tidal CO2!! This is a talk that you NEVER knew you needed until you hear it. Trust me, this is 45 minutes your patients cannot live without!
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS
Clinical Pearls (assisted by Dr. Lino Rafael O. Trinidad)
#1 concept: Will be the first warning of trouble in a struggling patient!
Capnography → LEAVE IT ON!! If esophageal, will go BACK to purple
- Is the immediate picture of ventilation (SpO2 delayed)
- Hypoventilation occurs 1-2 minutes before hypoxemia
- Ways of Measuring (Is the LAW for conscious sedation)
- POC addition to ETT (standard intubation equipment)
- Sidestream- can add dead space; can underestimate CO2
- Mainstream- T-piece adaptor at the airway opening; does not add dead space
- Mass Spectrometry- CO2 eliminated / O2 consumed
CO2 Waveform
- Evaluate for:
- Height
- Frequency
- Rhythm
- Baseline
- Shape
- Systematic Approach
- Is CO2 present (waveform)
- Is the baseline zero
- Evaluate the:
- Expiratory upstroke: steep, sloping, prolonged
- Expiratory (alveolar) plateau: flat prolonged, notched, or sloping
- Inspiratory downstroke: steep sloping or prolonged
- Just read the number
- Check ABG (Try to match the PaCO2, if its not within 5 a problem)

- Alpha angle: amount of V/Q mismatch
- Beta angle: if >90 degrees → rebreathing occurring
Evaluation of waveform abnormalities:
- Waveform regular shape
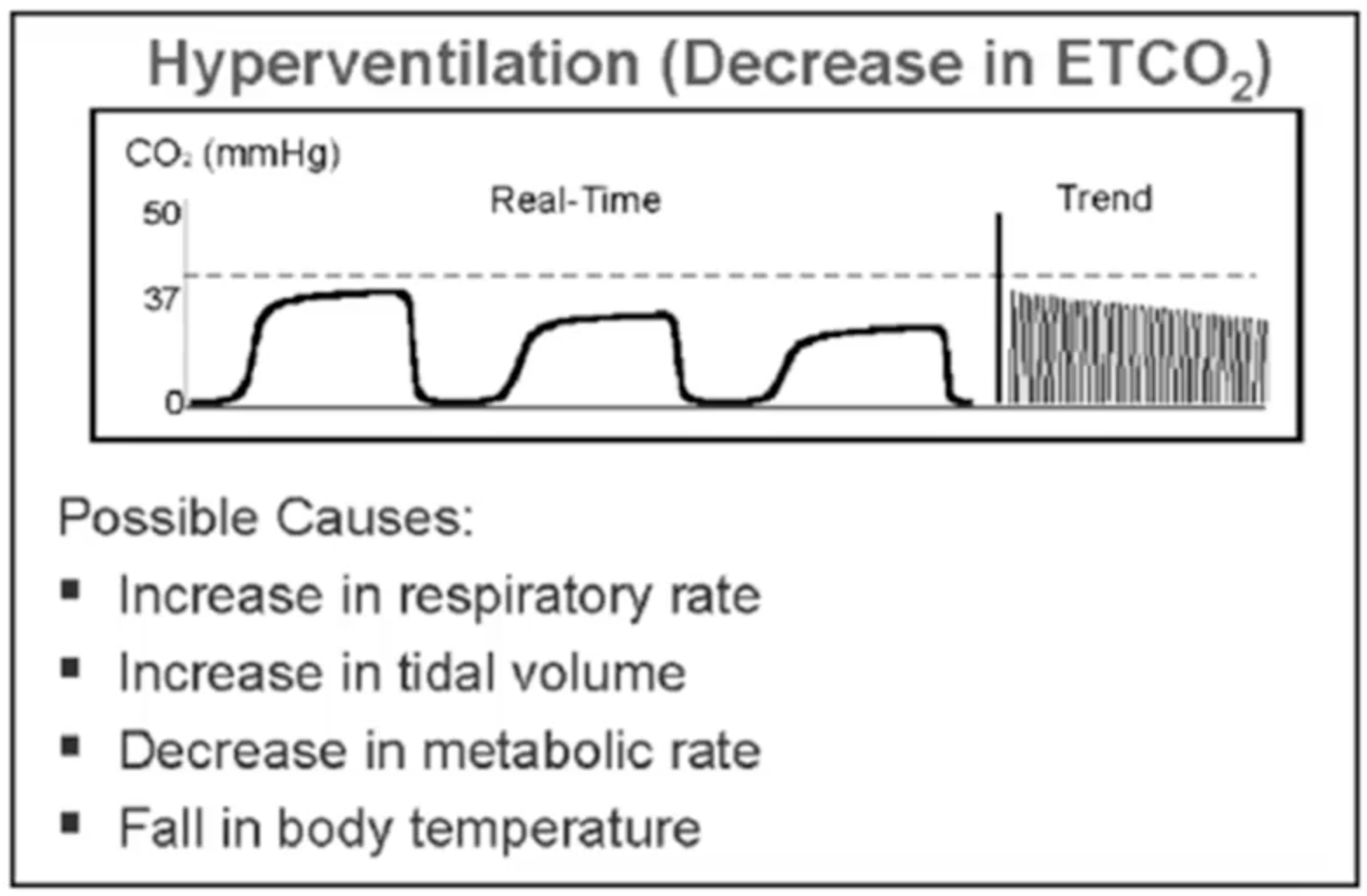
- Plateau below normal = CO2 deficiency
- Hyperventilation
- Decreased pulm perfusion
- Hypothermia
- Decreased metabolism
- Plateau above normal = CO2 excess
- Hypoventiltion
- Absorption of CO2 during laparoscopy
- Fever
- Dietary excess
- Sudden increases: sodium bicarb use, release of tourniquet
- Watch for Trends:
- Plateau below normal = CO2 deficiency
Special uses:
- Assessing Intubation and Ventilation
- 100% specific
- Facemask can force some pharyngeal air into stomach
- Esophageal intubation may be positive for CO2 (usually less than 10, decreases over breaths)
- Watch out for plug, kink, apnea, severe bronchospasm
- 100% specific
- ETCO2 and CO
- CO largely affect ETCO2 in dynamic situations, not when stable
- ETCO2 < 10 after 20 mins of CPR associated with a very high mortality
- Must make sure adequate compressions before judging ETCO2
- Dead Space i.e. Altered CO2 clearance
- Hypercapnea with adequate ventilation implies dead space
- Bohr-Enghoff Equation; Dead space = (PaCO2 – PECO2) / PaCO2
- Normal dead space is 2ml/kg
- Can be also calculated via Volume Capnogram
- Ventilator Adjustment
- Increase PEEP if gradient too high
- Useful for weaning vent once gradient is established
- Measure ETCO2 every time you get ABG
- Increase PEEP if gradient too high
- ARDS (?Dead Space Disease)
- TV distributed to poorly or non-perfused parts:
- Microemboli
- Endothelial damage
- Non-survivors have higher dead space, can be prognostic
- Serial measurement of deadspace for progression
- TV distributed to poorly or non-perfused parts:
- PE
- Hypoxia, clinical scenario
- 13-20% drop in dead space = CTA immediately
- Good NPV (100%); PPV (66%)
- Ventilator Weaning
- Obtain a gradient every AM (Volumetric would be more helpful)
- ETCO2 + RSBI is indicative of the proper score for extubation
- VA ECMO Weaning
- ↓ECMO flow by 40% → ETCO2
- ETCO2 will changed steeply with a flexion point (good symbol of coming off VA ECMO)
- ↓ECMO flow by 40% → ETCO2
Suggested Reading
- Checketts MR, Alladi R, Ferguson K, Gemmell L, Handy JM, Klein AA, Love NJ, Misra U, Morris C, Nathanson MH, Rodney GE, Verma R, Pandit JJ; Association of Anaesthetists of Great Britain and Ireland. Recommendations for standards of monitoring during anaesthesia and recovery 2015: Association of Anaesthetists of Great Britain and Ireland. Anaesthesia. 2016 Jan;71(1):85-93.[PubMed link]
- Thomas AN, Harvey DJR, Hurst. Standards for Capnography in Critical Care – The Intensive Care Society Guidelines 2014. [ICS Link]
- Nassar BS, Schmidt GA. Capnography During Critical Illness. Chest. 2016 Feb;149(2):576-85.[Pubmed Link]
- Monnet X, Bataille A, Magalhaes E, Barrois J, Le Corre M, Gosset C, Guerin L, Richard C, Teboul JL. End-tidal carbon dioxide is better than arterial pressure for predicting volume responsiveness by the passive leg raising test. Intensive Care Med. 2013 Jan;39(1):93-100.[PubMed Link]
